
 Loading...
Loading...
Literature review report – Youth Risk Perception and Decision-Making Related to Health Behaviors in the COVID-19 Era
Loading...
 Loading...
Loading...
 Human Development has added two new faculty members this year, Misha Inniss-Thompson and Adam Hoffman. Click here to read more.
Human Development has added two new faculty members this year, Misha Inniss-Thompson and Adam Hoffman. Click here to read more.
 The Bronfenbrenner Center for Translational Research (BCTR) is launching a new project – the Community Neuroscience Initiative, (CNI) headed by four Human Development faculty, Anthony Burrow, Marlen Gonzalez, Eve De Rosa, and Adam Anderson. All have been engaged in STEM outreach and engagement and envision CNI as a way to build connections between neuroscience research, STEM education, and community empowerment. Click here to read more.
The Bronfenbrenner Center for Translational Research (BCTR) is launching a new project – the Community Neuroscience Initiative, (CNI) headed by four Human Development faculty, Anthony Burrow, Marlen Gonzalez, Eve De Rosa, and Adam Anderson. All have been engaged in STEM outreach and engagement and envision CNI as a way to build connections between neuroscience research, STEM education, and community empowerment. Click here to read more.

Concussion injuries among high school and college athletes have become a central concern in youth sports. Prompt self-reporting of a concussion immediately improves brain recovery and is necessary to reduce second-impact syndrome, rapid swelling of the brain after a person receives a second concussion before symptoms of the first concussion have subsided. Unfortunately, repetitive head injuries in adolescents and young adults are often underreported. Peter Ajayi, HD’19, David Garavito, JD/PhD ’21, and Valerie Reyna, professor of human development, are the first to detail an association between socioeconomic status (SES) and concussion reporting intentions among adolescents and young adults. Click here to read more.

Despite the restrictions on campus to prevent the spread of COVID-19, graduate and undergraduate students in Human Development persisted and excelled in their research and outreach activities. Click here to read more.

Concussion injuries among high school and college athletes have become a central concern in youth sports. One of the most important decisions an athlete can make is whether to report a concussion to the coach. Prompt self-reporting of a concussion immediately improves brain recovery and is necessary to reduce second-impact syndrome, rapid swelling of the brain after a person receives a second concussion before symptoms of the first concussion have subsided. Unfortunately, repetitive head injuries in adolescents and young adults are often underreported. Peter Ajayi, HD’19, David Garavito, JD/PhD ’21, and Valerie Reyna, professor of human development, are the first to detail an association between socioeconomic status (SES) and concussion reporting intentions among adolescents and young adults. (https://onlinelibrary.wiley.com/doi/10.1002/bdm.2235).

Dr. Reyna and her students incorporated Fuzzy-Trace Theory (FTT) (Reyna, 2012) into the research to capture important unexplained variance in the self-reporting of concussions. According to FTT, when people make decisions, they process the information in two ways, as "gist," or its bottom-line meaning, and "verbatim," or its superficial details. The gist and verbatim formats are encoded and retrieved from memory separately. Gist processing is a more developmentally advanced form of reasoning that reflects education, culture, beliefs, and other life experiences. As people age, they increasingly rely on gist, rather than verbatim, processing of information which leads to healthier intentions and behaviors. Although adolescents and adults process information as gist and verbatim, adolescents are more likely to rely on verbatim processing and the finer distinctions of the tradeoff between risks and rewards when making decisions (e.g., "The chance of something awful happening to me is very low, so I can take a chance.") whereas adults are more likely to rely on a simple, qualitative categorical gist of risk (e.g., "There is a chance of a catastrophic outcome, and I should avoid putting myself in harm's way at all costs.")
This is the first study to propose and demonstrate a link between SES and reporting intentions. They hypothesized this connection because of putative effects of SES on cognitive development, namely, on gist processing. Based on FTT, categorical gist processing and gist principles of risk avoidance are predicted to develop with experience from childhood through adulthood and to promote healthy decision-making. Low SES, they posited, offers fewer opportunities for enriching experiences, on the one hand, and greater exposure to stressors, on the other hand, delaying cognitive development. This is consistent with previously reported SES differences in gist processing. Consequently, they expected that SES operating through gist processing, such as the categorical insight that a concussion can produce life-altering brain damage, would be associated with higher reporting intentions. High-school and young adults in their study completed a survey about concussions and sports. Overall, for each of the two age groups, and for athletes as well as nonathletes, SES was associated with reporting intentions. It was the responses to questions on gist processing, concussion knowledge, and healthier attitudes about concussions that were each associated with greater intentions to report concussions. Ajayi, Garavito, and Reyna conclude in their paper that although educational initiatives currently focus on rote knowledge of concussions and healthy attitudes to reduce the underreporting of concussions, they recommend that future interventions use gist to communicate risk, especially to low SES youth by adapting successful FTT-based risk-reduction curricula from other domains.
Peter Ajayi received a post-baccalaureate, NIH Intramural Research Training Award to study the myofibrillar and mitochondrial networks within skeletal muscles using advanced imaging methods at the NIH National Heart, Lung, and Blood Institute. He is currently attending Warren Alpert Medical School of Brown University.
David Garavito received his J.D. from Cornell Law School in 2020 and received his Ph.D. this year from the Law, Psychology, and Human Development Program at the Laboratory for Rational Decision Making at Cornell University. His research examines the perception of risks and risk-taking within the context of sports and the cognitive and neural effects of concussive and sub-concussive injuries.
 Valerie Reyna leads discussions about communicating the risks of COVID-19 to the public.
Valerie Reyna leads discussions about communicating the risks of COVID-19 to the public.
 Karl Pillemer of the Cornell Reconciliation Project writes about how the COVID-19 crisis has led some people to reconcile with their families.
Karl Pillemer of the Cornell Reconciliation Project writes about how the COVID-19 crisis has led some people to reconcile with their families.
 Qi Wang articulates the role of cultural psychology in bridging cultural gaps in psychological research and in society.
Qi Wang articulates the role of cultural psychology in bridging cultural gaps in psychological research and in society.
 Marianella Casasola shows how multisensory play in naturalistic settings is fundamental to the early development of visual-spatial abilities.
Marianella Casasola shows how multisensory play in naturalistic settings is fundamental to the early development of visual-spatial abilities.
 Wendy Williams and Jane Mendle contribute to our understanding of the career challenges women in academic sciences face and the way forward.
Wendy Williams and Jane Mendle contribute to our understanding of the career challenges women in academic sciences face and the way forward.
 Valerie Reyna, Lois and Mel Tukman Professor of Human Development, Director of the Human Neuroscience Institute, and Co-Director of the Center for Behavioral Economics and Decision Research, was invited to moderate the symposium “Responding to COVID-19: Emerging insights from social, behavioral and economic sciences,” for the National Academies of Sciences, Engineering, and Medicine. You can watch the video recording below:
Valerie Reyna, Lois and Mel Tukman Professor of Human Development, Director of the Human Neuroscience Institute, and Co-Director of the Center for Behavioral Economics and Decision Research, was invited to moderate the symposium “Responding to COVID-19: Emerging insights from social, behavioral and economic sciences,” for the National Academies of Sciences, Engineering, and Medicine. You can watch the video recording below:
Refer to Dr. Reyna's publications to learn more about her Fuzzy-Trace Theory approach to decision making about COVID-19 risk:
Reyna, V. F. (2020). A scientific theory of gist communication and misinformation resistance, with implications for health, education, and policy. Proceedings of the National Academy of Sciences of the United States of America. Advance online publication. https://doi.org/10.1073/pnas.1912441117
Reyna, V. F. (2020). Decision making about risk in the era of the novel coronavirus disease. CHEST, 158(4), 1310-1311. https://doi.org/10.1016/j.chest.2020.07.005
Reyna, V. F. (2020). Of viruses, vaccines, and variability: Qualitative meaning matters. Trends in Cognitive Sciences. Advance online publication. https://doi.org/10.1016/j.tics.2020.05.015
Dr. Reyna also chaired the symposium, "Theories of medical decision making: Explaining, predicting, and improving health and healthcare" at the 42nd Annual Meeting of the Society for Medical Decision Making. You can watch the video recording below:
Newswise Live Expert Panel discussion of unique angles to the COVID-19 outbreak of interest to the public and the media, including public health, testing, business and financial markets, 2020 elections, and more. https://www.newswise.com/articles/covid-19-exploring-the-unanswered-questions-with-newswise-live-expert-panel
The following is a transcript of the Newswise Live Expert Panel on Thursday, March 12, including the following experts:
Thom Canalichio: Welcome, everyone, my name is Thom Canalichio here at Newswise, and this is one of our Newswise live expert panels. So we've invited these five wonderful experts from several different universities and other organizations that are working with us to be available today to talk about the coronavirus and the COVID-19 outbreak that's currently happening. We have experts on topics related to health and medicine, as well as things like psychology, history and business, to try to answer a lot of questions that they feel should be discussed in the media more widely and give our media participants here logged in an opportunity to ask questions.
So a reminder again, for the media who are logged in, please, chat any questions that you have directly to me, or feel free to chat it to the whole room and as we go through the process, I will relay those questions to our experts. We'll start with a couple of questions for Dr. XinQi Dong and then move on to another expert with breaks to invite the media to ask further questions. Well, we have some prepared already to kind of get things going and then we'll certainly circle back to everyone again at least one more time and try to see if there's any discussion amongst our experts that they'd like to respond and build on what each other are saying, we'd certainly find that interesting if that can happen.
So without further ado, I want to introduce Dr. XinQi Dong from Rutgers University. Dr. Dong I believe is an expert in epidemiology among many other topics. So I'd like to ask Dr. Dong if you can talk a little bit about what we know about the COVID-19 and Coronavirus and the contagion factor. This is something that's been covered a lot in the news and I don't think there are clear answers yet, but maybe you can point us in the right direction about how long someone may be contagious, about the virus, surviving on various surfaces and how we measure and monitor what infection rate may ultimately look like as that happens. What could you tell us about that Dr. Dong?
Dr. Dong: Thom, thank you for hosting this and for Newswise as well and to our esteemed colleagues. My background, I'm a geriatrician by training and epidemiologist and I direct the Institute for Health Care Policy and Aging Research at Rutgers University. COVID-19 virus, you know, this pandemic, there are various different hypotheses, we really don't know as much as we ought to know. Some of the things that we do know that this is, you know, contracted by close contact proximity for people coughing, sneezing, bodily fluids, and really are factors that drive the communication of the spread and when you look at or rather that the factor that drives the spread of one person to the next set of person, those numbers are quite a bit of variability as well. So you know, when you look at a comparison to other SARS, MERS, and Influenza related viruses, really we don't know what our denominator really is in terms of percentages and mortality and the risk for spreading.
However, I do think that despite all of this, how we measure, COVID-19virus and how we detect it are really important. I think, having social distance it is something that we've been suggesting to our patients, if you're sick call your physician first, before you come to the clinic, especially having a specific set of symptoms; you know, high fever, cough are some of the symptoms that we often talk about but the geriatric patients, are not often the same as, for example, in older adults, they may not be up to [Inaudible 03:44] the high fever as a younger adult or a child who may be able to. So signs and symptoms are really different and I think keeping the healthcare providers' family being cognizant of that it's really an important factor to understand the difference between what's an allergic reaction, what's COVID-19and what's influencing that. Social distancing is something that we really have been recommending especially for those with co-morbidities, people with lung disease, people with diabetes and people with underlying immunocompromised conditions, and really to reduce the spread of the virus as well. In terms of detection on surfaces, Thom, it's a bit of a controversial question in the sense that just because we measure a fragment of a virus or bacteria on the surface does not necessarily mean that's infectious per se. A typical example that I give to patients is that if you look at the treadmills you can often consider them some of the most contaminated places does not necessarily mean it's the most infectious because bacteria and virus can only live outside of the host for so long and just because he detects protein fragmentations does not necessarily mean they're contagious in nature. Let me pause here.
Thom Canalichio: Thank you, Dr. Dong. I want to dig into a little bit more about some of the questions on geriatric patients and others who might be at risk because of age and other immuno-compromised conditions. I want to remind our media participants that you can submit questions on the chat, and we'll relay those to each expert. So I want to give Dr. Dong a chance to answer a little bit more about that. If you can describe what are some of those conditions that might cause a patient to be immuno-compromised? And what are some of the strategies for prevention as well as treatment of those? Obviously, there's no cure specifically for this disease, that's been mentioned pretty widely in the news, but treatment in terms of supportive care, I understand is the name of the game so what can you tell us about those concerns?
Dr. Dong: Sure, thank you in terms of the prevention and treatment, and well let me get to the vulnerability, anyone with, for example, with ongoing pulmonary disease like Emphysema, as Diabetes, people who have history of cancer, who are taking chemotherapy, people with immunological conditions, such as Hepatitis or, you know, Lupus, or take medication that suppresses immune systems, they're really those are the patients who are the most vulnerable as well and I think in terms of prevention, really, I think, as you've heard, again, and again, wash your hands and sing two Happy Birthday equivalents, to be able to clean your hands and we think about social distance, recommending in a one and a half arm's length from the people next to you, but in elderly patients are very different because often they're the people who are mostly in need of care and especially for elderly who have needs for activity of daily living, they need dressing help, feeding help, going to the bathroom, and when a nurse's aide or a family member comes into the house, they really should be washing their hands and wearing gloves and trying to have the same people come into the house all the time, so you know whether that person is having symptoms over time. The mounting of fever and the immune system are things we do need to consider because the elderly as I said earlier may not mount the same fever or the immune response may be different. As you get older, your immune system does weaken as a sort of a normal part of aging and I think really needs to be taken into consideration, treatment in terms of treating symptoms, and I think the most important thing, Thom is to differentiate between what is a factor in pneumonia, what it's viral pneumonia, what is allergic rhinitis? What is a flu, for example, and understanding the signs and symptoms really the most important point of thinking about treatment because, for someone that's really having a high fever, having lower respiratory symptoms, that's short of breath, you don't want them to stay home, you actually want them to call their physicians and to understand this outside of the norms, of the symptom that he or she experiences as a respiratory symptom and when they should be tested and those are really important questions to consult with the healthcare providers.
Thom Canalichio: Thank you so much, Dr. Dong, any other questions for Dr. Dong from our media participants, please chat those and when we circle back around, we'll relay those to him and have him answer. I'd like to move on next to Dr. Ali Khan from the University of Nebraska Medical Center. Dr. Khan is an expert on public health and infectious disease in a number of other topics and I'd like to invite you to answer some questions now to Dr. Khan. Thank you so much for joining us.
Dr. Khan: Thank you, Thom, and as a little bit of a way of introduction. So I spent 20 years at CDC, chasing SARS and other highly contagious infectious diseases detailed that book Work in the Next Pandemic and here at the university, we've been receiving patients for weeks now from the Diamond Princess and other sites since we're the premier biocontainment unit in the United States.
Thom Canalichio: As many people may recall from the Ebola crisis just a few years ago, the University of Nebraska Medical Center was one of the main places where patients were being sent when they were brought to the US for treatment. With your knowledge about, obviously your own medical center, as well as the hospital system at large. Dr. Khan, how do you assess the capacity for a large volume of admissions if the infection rates were to spike? What's our capacity there? And how are hospitals preparing?
Dr. Khan: So we're clearly unprepared and we don't even need to talk about a pandemic during a really bad flu year, we know that we see ER and hospital diversions because we can't handle a really bad flu year in the United States, let alone this pandemic. So our main focus is on helping healthcare prepare for a potential flood of patients. So what they're doing is they're looking at those two scenarios. How do I take care of patients coming in the door, make sure we do it safely. Let's not infect our healthcare workers, not infect any other patients in our hospital and then also, how do we make sure that in addition to one or two coming in, if dozens of patients came in, how do we take care of them and we already see healthcare as being very proactive and innovative in approaches. So for example, one of the key things we want to do is make sure that we identify and isolate patients very early and Dr. Dong was very eloquent talking about calling your doctor beforehand when you come into the ER so they know that you're coming but some ER's have now sort of started screening people even outside the emergency room in the hospital, so they can quickly triage them based on where they need to go and they're less likely to infect other people. We know hospitals in Washington are already doing Doc drive through testing of their healthcare workers, which is now being extended to other people. So you don't have to go to a healthcare setting to get tested because a) if you're infectious, we don't want you to infect anybody else and b) if you're absolutely fine, we don't want you to get infected by somebody else who's in the healthcare setting. So these are all the conversations going on across America to get ready for a potential flood of patients coming in.
Thom Canalichio: And what would you say would be the best course of action based on the current numbers and infection rates that we should start doing here in the US? And would you think that something along the lines of a kind of lockdown that was just announced a few days ago in Italy, would be effective and that now might be the right time to take those sorts of actions?
Dr. Khan: So what we need to do in every community in America based on what disease looks like in that community, is think about what are called non-pharmaceutical interventions, or social distancing is a colloquial term for that, so what we're trying to do is slow the spread of disease into the community and spread it out over a longer time and what that does a couple of things. So if you slow that large increase in cases, that's less likely to be a burden on hospitals, which is important and if you spread it out over time, you're giving public health time to do what they need to do to try to contain this disease and you're also buying yourself time for potential vaccine or therapeutics or drugs in the future.
Thom Canalichio: Thank you, Dr. Khan. If anyone has any questions for Dr. Khan, please chat them to us. I want to move on next briefly to Zhaohul Chen, who is a Professor at the University of Virginia Macintyre School of Commerce, to talk about a couple of topics related to business in the global economy. Thank you for being with us, Zhaohul Chen.
Dr. Chen: Thank you, Thom
Thom Canalichio: I want to ask you to tell us a little bit about what your knowledge is of the Chinese economy, and in particular as they really clamped down to get the outbreak under control. We saw their stock market; in fact, rise and I think you have some interesting views about that. Tell us what your take is on how we can assess the response of the Chinese economy and the Chinese government.
Dr. Chen: Sure, so as we know that this disease started in China and is still going on, even though the report comes to us that this situation is getting much better, but still people are suspicious of the accuracy and maybe we worry that the government may actually underestimate the severity of this disease. Having said that, it's clear that the government made a choice, rather than sort of stop or slow down the spread of disease, they actually chose another direction that is to make everybody to go back to work, okay? So that may, by the conventional wisdom, make the spread of disease worse but on the other hand, you have to go back to work to keep the economy growing again and most of the household activities run out of money and some do need to work or do basic jobs that have to sort of come back to work and the rate of recovery, some estimate is about 60/70%, so the economy is [Inaudible 14:40] come back.
And the government to help that in the sense that they are pumping a lot of money into the system, into the banking system or give money to the state-owned big companies; as a result, because at this stage, the money is not needed in manufacturing because the money's not the key problem, the key problem is that people want to work here. So to park the money into the stock market and elsewhere, so we see that the stock market is well, even though the economy is contracting, so this is what we see as strange things happening.
Thom Canalichio: If anyone else has any questions for Zhaohul, please chat them to us. I wanted to ask you also what you can tell us about what we've seen this week, obviously with a lot of stock market volatility and energy markets, in particular being predicted may be affected as there was some controversy with OPEC and oil pricing as part of this, obviously China a big energy consumer with their economy slowing down temporarily at least their demand for energy was lower. How do you see that whole picture shaping up? And what that might mean for the US economy and the global trade overall?
Dr. Chen: Sure, okay. So the breakdown of negotiation between Saudi and Russia, so this is what happened on Monday and that sort of wreaked havoc to their stock markets and capital markets in general. So the reason, in my view, is really sort of short term and is motivated by factors other than economics or business factors. So in my view, I think Putin has no incentive to give up at this juncture because he is seeking to change the constitution. He wants to be the President until at least 2030. So on the other hand, The Crown Prince of Saudi Arabia also has its own political problems because he wants to be the next successor. At this point, he really needs to appear strong and firm as a super-strong leader. So both of those leaders have all the incentive in the world to appear strong and cannot compromise because they don't want to appear weakened and cannot change the landscape of politics. As a result the head bursts completely, so this is over, they don't want to compromise. In the past Russia and OPEC almost always, you know, in this situation, try to negotiate and compromise, and in the past, mostly they'll work well, but at this particular juncture, they cannot, okay? Because they cannot afford to compromise, they have to appear strong. So the topic down on economic habit have sort of spilt over, but it's okay in the sense that both Countries can afford at least the short term to have this sort of chaotic, okay, they can have some deficit and they can take some hit in the oil revenues. In particular, Russia, Russia has been sanctioned by the west for a long while so they can sort of weather the storm a little bit. So I think it's going on a little bit but will not have a long term impact, because I think eventually they'll come back to the negotiating table again and solve this issue.
Thom Canalichio: So, Zhaohul, we have from Mark Manier: “A key part of leadership in a health crisis would be projecting confidence and relaying accurate information and reasonable policies, the Trump administration record has been mixed on this front. Could you comment on last night's speech by the President if you followed that closely enough that you feel like you can; and for example, blocking travel from Europe, was this adequate, too little or too late?” And I'd love, Zhaohul, for you to answer that. I'd love to also have Dr. Reyna answer that.
Dr. Chen: So, all I can comment here is the reaction of the stock market today, as we know that the European and American economies are close, very intertwined. So the stop of the travel is going to be a big blow to the economy. Today we have, at least in the early morning; at least, we have like, almost close to a 10% decrease in the stock market. Now it's about...it's down a little bit more than 2%, so it recovered a little bit. The investors worry about, that the policy, this sort of stop [Inaudible 20:48] may cause more harm to the economy than, actually, the disease itself. So, people really worry about the uncertainty in terms of the government policy because, okay let's just make just a crude and cold sort of a calculation. So the death rate, let's see, assume it's 2% and most of the concentrates are older people. So those are like retired people and are maybe less productive. As a result, in fact, to the GDP growth or the whole economy, it's not as even though with that play out, as it is, so mostly the stock market does come from the uncertainty in government response.
Thom Canalichio: I want to go next to Dr. Valerie Reyna of Cornell University. Dr. Reyna, I think, with your background, talking about risk perception and a lot of other topics related to that, I think it'd be very interesting for you to weigh in as well on your assessment of President Trump's address last night. Dr. Reyna is from Cornell University where she's in psychology. Tell us your views on that in response to Mark's question.
Dr. Reyna: I'm in the Human Neuroscience Institute and direct the center on behavioral economics and decision making and thank you so much for doing this and getting the word out, obviously, information is so important. It's difficult for me to comment on the President's address, but I can certainly comment on as a scientist of the psychological components here. I was struck in all of the comments of the experts so far, how contingent everything they've said is on human behavior. Human Behavior really is the linchpin here, whether we're talking about the reactions of the market, which seemed to be very psychological or we talk about non-business causes and non-pharmaceutical factors. We're talking really about Psychological Science and Human Behavior. So with any virus, whether we're talking about HIV or HPV, the Human Papilloma Virus or the Coronavirus, human behavior is key and there's a science of that, that's extremely instructive. So people are getting lots of information from many places. They're getting it from social media and that spreads enormously quickly. They're getting it from family and friends. They're getting it from new sources like this one and this is really, really important. I can't say, I can't tell you, I can't overestimate how important it is to get the news out to people and to continue to repeat it but people are awash in information and a lot of it is misinformation. So they're struggling and what the psychological literature says they're struggling to figure out what is the gist of the information? What does all of this boil down to, our own models of risk communication really relied on the computer as a metaphor for human thinking but people do not think like computers, they don't just take in a whole bunch of facts and fill up with facts and then retrieve the facts, they interpret the facts, so it's extremely important, and this is the foundation for our emotional reactions to the facts as well. When we interpret the facts, it's called cognitive appraisal. We decide whether Is this a threat, should I feel fearful? Or should I feel relief? And you have certain paradoxes right now in the information that's coming at people. People are in a quandary over whether they're in a low-risk situation, or they're a high-risk situation and it's confusing, and it's confusing in a way that is true many public health threats. On the one hand, if you look at the absolute number of deaths so far, and people talked about the denominator out of these large populations, many people will say; ' That's low risk because there are a few people who've died out of large populations'. On the other hand, we know that this is changing rapidly and so if we think about the prevention and mitigation of this pandemic, this is going to rise rapidly. So the actions we're taking now are because we perceive high risk, but we're not perceiving, it's not necessarily at the present moment, it's what's going to happen very soon. So the experts are sort of saying two different things to people and naturally, people are confused but the bottom line is, this is going to change, these cases are going to increase, from a few today to many tomorrow, as Dr. Falchi said yesterday, and that's really the gist that we have to stress that even though the number of known cases at the moment around you may be small, the nature of epidemics is that there's a cumulative probability mounts up really fast and it mounts up much faster than people can apprehend.
Thom Canalichio: We have a question from Freelancer Kathy Kowalski asking about the impacts of social distancing? And what are some of maybe the barriers to people implementing those things in their lives, especially where it might involve family with members who are older and have these immuno-compromised types of situations? What are, in your view, the complications to people taking action on the right steps that they should take in their personal lives, so that they could protect their family members, especially in a case for example, where they might be compelled to travel, to visit family who maybe don't live in the area or things like that, how does that break down and people take the gist of the risk and then start changing their own behavior?
Dr. Reyna: Well, you said it, I mean, the people have to make decisions and this is where the science of risky decision making is so fundamental. They have to absorb all this information and make decisions as an individual and that will then determine how they process that information, will determine their actions and their emotions. So, and there are some really predictable things that are difficult to understand. For example, young people may be vectors of this, meaning that they're infected, and they're spreading it to lots of people, so they themselves may not show symptoms as severely or as soon as older people. So you have people who, and this is true, by the way in the ordinary flu season as well, people spreading the disease and then people vulnerable to the disease. So you have to think about, again, two different things that almost seem contradictory and in making people's decisions, they need that information.
Thom Canalichio: Thank you, Dr. Reyna, for some historical perspective, I want to go now to Dr. Tom Ewing of Virginia Tech, and ask him to tell us a little bit about some historical examples, for example, Dr. Ewing, compare the COVID-19 outbreak to the 1918, Spanish Flu or even something a little bit, maybe less well known the Russian Flu in the late 19th century, and how the actions that officials took in those situations can give us a template for how we can maybe make better decisions today.
Dr. Ewing: Sure, thank you and I am going to echo my colleagues in thanking you for arranging this forum and giving us the chance to participate but also more broadly to be able to disseminate information that is useful more and more widely. There are many, many parallels to the 1918 influenza epidemic, particularly around the question of social distancing, non-pharmaceutical interventions, many of the things that we're experiencing right now, closing schools, banning public meetings, trying to limit travel, taking steps to ease congestion in public spaces. Most of those were implemented in the United States strictly in the cities in the fall of 1918, and so I think we can look at those examples in a couple of different ways. One is to say, what was the point in the epidemic at which they were implemented? Was it just the right time? Was it too late? Was it too early? How effectively were they announced, enacted? Where they were they completely implemented or were they partially implemented? And then to go back to this question of psychology, how do people respond to these kinds of measures and you can see a real spectrum of responses in the 1918 influenza epidemic in the United States. Things like the decision to close schools which a lot of school systems are dealing with right now, was pretty widely adopted in 1918 across the United States. In some cases, this was done early enough so that the children were kept home and they did not spread the disease as widely as might have happened, and in other cases, it was probably done too late, the disease was already in the community, it was already spreading and at that point closing the schools doesn't really do any good at all. In fact, it could make the situation worse by dispersing children back into their, into their families and out into the community and other ways, but it's interesting in 1918, there were some schools and very large school systems that actually chose not to close the schools. New York City and Chicago are two of them, with the argument that you also hear now, which is the schools themselves may be a safer place for children. There you could practice pathogenic practice activities there. You can screen children and see if they're sick and in some ways you can provide social services and so I think the historical example of the 1918 influenza epidemic gives us a kind of range of ways to think about the current one, we can look at situations in which correct decisions were made that were implemented that may have made a difference in terms of slowing the spread of the disease and lessening its impact, but there are plenty of counter examples, you know, situations where social distancing practices were not implemented, and there was the disease spread much more quickly and became more deadly as a result, or where they were implemented too late or very partially, and one example, you can actually hear less about it now than you did a couple weeks ago, was a whole question of wearing masks, there are cities in United States, San Francisco, in particular that made it mandatory to wear a mask out in public, those measures probably didn't help at all, the masks were not effective in containing the spread of disease, and what they actually did was to provoke people into a kind of resistance, they didn't want to wear the mask, and so they didn't, and so I think that we have to be very aware, as we implement public health measures, to think about the timing, to think about how they're being enforced, how widely and how are people going to react to them.
Thom Canalichio: Thank you, I'd like to start back again to Dr. Dong as well as Dr. Khan to ask about the announcement made last night from the Trump administration regarding the 30 day travel ban from Europe. This was part of Mark Mainers question about responses to Trump's National Address last night. Dr. Dong would a measure like this, in your view, first of all, be the right step at the right time and ultimately be effective and do you think maybe we should be doing this with wider regions of international travel?
Dr. Dong: That's a good question comments Thom, it's really difficult to decipher and the one reason is that is because there's a community spread as Valerie said that there are many vectors, people who are fairly asymptomatic who already traveled across the globe and so it's really not clear shutting the border or limiting travel can achieve the same benefits, as I think that one may hope for, but I think the better question is really how do we empower patients and families and community to adopt those hygiene practices and to really change your behavior that we have so used to for years and I think the last three months really forced us to think about how do we need to act differently? How do we behave differently in our day to day lives to minimize the spread? I think the core responsibility, as much as the government and the systems can play a role really resides to each one of us and how we spread this news and what's the right thing to do for our peers and families.
Thom Canalichio: Dr. Khan, what's your view about the announced travel ban from Europe and where else should we be considering to ban travel and what ultimately might be the effect of this?
Dr. Khan: So thanks, Thom, as you know travel bans are a political lightning rod. So I'll stay away from the political lightning rod and stick with the science for now, so a travel ban associated with a clear strategy around containment is the model that we see from China. So China had a clear strategy that they want to contain and as they liked, I think, as President Xi likes to say; 'Gonna beat back that devil virus into the wild'. So they've gone from 5000 cases to 20 to 40 cases a day and now what they're doing is in Beijing specifically, international visitors to Beijing must undergo a 14-day quarantine if you're coming into Beijing. This is sort of variably enforced throughout the country at this point may eventually go countrywide. So China has decided it's not called a travel ban, but it's essentially the same thing, right, which is, they've gotten rid of disease within their country, or they almost have gotten rid of it and they're not anxious to import any back end at this point from somebody else.
Thom Canalichio: Thank you, Dr. Khan. Dr. Reyna, what is your impression of the acceptance more widely around the US or around the world of things like these travel bans? As people categorize their perception of the risk, right? Are they potentially becoming more inclined to either voluntarily limit their movement around or accept if it's imposed by the government? What are your thoughts on that?
Dr. Reyna: Well, again, it's all hinges on people's understanding of why the travel ban might or may not be effective, what exactly is it trying to do? and again, this distinction between containment at the initial stages versus spread at later stages is very important. So these policies have to be explained to people. The other issue is that any risk is perceived as more dreadful if you can't control it personally. So control and personal control of your risk feeling that you're out of control is been a long-standing classic dimension of risk perception, risk communication and reaction to risk. People need to feel that they can take the protection, their actions they can take, and when you control people's behavior and tell them they can't do things and you see this for example, in the vaccination controversies, which is going to be an issue obviously when we develop a vaccine for the Coronavirus, some people feel if the government is telling you that you must take a vaccine that gets people's back up. So, we have to explain to people, at the end of the day, we have certain policy tools, we can quarantine we can, the government can do certain things, but it helps enormously when you're talking about millions of people, that they understand why the government is taking certain action and that they feel personally empowered.
Thom Canalichio: And what would you say about for example, in an academic community or university campus and the decision to halt classes, or hold all classes online, but no classes in person, as I believe a number of universities are announcing each day as this progresses. One of the questions from our attendees, it touched on concern about anxiety and social distancing among college students, as a precursor to mental health concerns as well as other things. What's your take on how we can better communicate to university communities, for example, to mitigate those issues, as even though their lives are getting disrupted?
Dr. Reyna: Yes, I think it's very predictable that people are going to feel more socially isolated when they're more socially distanced that just goes with the territory and a lot of research has shown that that connection to other people is so important for health, mental health and physical health. So, however, we live in a wonderful age of technology, and for all the problems that social media and the other technologies create, they also create opportunities to connect to other people, to other human beings and we're now trying to take advantage of that and so people do not feel isolated. I also think people in their local communities need to reach out to people that there are older people living alone and so and think about your neighbors. So it is very predictable as these social cues mount, that there's something wrong when you cancel classes and people have to go home, when sporting events are canceled, that is going to provoke anxiety and when you have people more socially distanced they're going to feel more isolated and that's one of the coping mechanisms, there are other people who are dealing with fear and anxiety. So we have to think about that and be proactive and think of ways to connect electronically in other ways that can reassure people.
Thom Canalichio: Thank you. For Dr. Dong I would like to ask whether or not you think that social distancing at this stage, is it too late, are more drastic measures needed. This is from one of our reporters attending.
Dr. Dong: I'm sorry; I delivered some hearing, would you mind repeating the question?
Thom Canalichio: Yes, absolutely, absolutely. Is it already too late for voluntary social distancing to be effective in the United States? And how long would those kinds of measures such as working from home and kids staying off-campus how long would that be needed to be in place for it to be effective if it was going to work?
Dr. Dong: Sure, Thom, I don't think it's too late. I do think that especially looking at the trajectories of the viral spread that seems to be still going up. I mean, I think the potential mode and when that happens, I think the social distance does play a role, but I do want to acknowledge what Valerie said earlier about the unintended consequences of social distancing, especially for older adults, in the way that we know social isolation leads to premature death and all sorts of other mental health outcomes, that we ought to leverage other ways to be able to support the families and vulnerable populations. In terms of when do we decide to help that or reduce that I think all the factors that I talked about earlier are not [Inaudible 40:35] or are zero, essentially looking at the speed of the spread of the virus from one person to another and there are variant estimates of what that number is going to be, but I think until the numbers become really stable a bit, then I think there's a social distance does play a role and I think some of that does speak to the fear factor that Valerie talked about as well the unknown, right, unknown how that will impact me, my family people around me but it's not to say that we should just do a social distancing myself without acknowledging the unintended consequences.
Thom Canalichio: Thank you to Dr. Khan again, one of the questions from our reporters touches on a study being done in Germany currently of COVID-19and the results indicate that the virus may be still traceable in the patient in the form of the RNA, whether or not they're still contagious is not known. Are you familiar with this study? What would you say to exploring that question itself to try to determine the contagious period and other questions?
Dr. Khan: Glad to provide a little insight into that. So the data suggests that people are actually quite infectious very early when they start demonstrating symptoms and that maintains true for about five days or so before the virus decreases and then for most people, it's gone in about eight days and this is in their nose and in their mouth and so the upper respiratory part of their body. Now independent of that, we do know that you can find virus fragments and blood stool, urine, but they don't seem to be able to pick those up on virus isolation. So that's a little bit different than finding the live virus than finding pieces of the virus. So all of this is encouraging, some of it is discouraging news, which means that when you're mildly are just sick, that you are putting out a whole lot of virus, which explains why we're seeing such efficient transmission within our communities but the fact that it rapidly declines means that after about 10 days or so you're unlikely to be infecting other people. There are also additional studies that suggest that if you have a very mild or asymptomatic infection, you also likely are not shedding as much virus and are less likely to infect other people. So some pieces of good news in that, I remember the initial concern that the PCR was positive and stool and others and the urine and stuff like that but just to remind people that just because you have a fragment of a virus in a fecal sample does not mean that it's live, and also does not mean that this is a source of transmission. We know that people most likely are getting infected, as you heard from Dr. Dong earlier, from coughs and sneezes and stuff like that at short distances.
Thom Canalichio: Thank you. I want to ask Dr. Chen, again, about the impact to markets and the economy. We're seeing the Dow continuing to drop. I just loaded it on a browser here and it's down almost 2000 points at the moment. There have been continuing announcements about cancellations and major events being postponed, for example, we The NCAA Tournament coming up, I just noticed that UVA, my Alma Mater, our basketball game against Notre Dame is canceled. How would you predict? How would you analyze the impact of these kinds of things to the economy in the United States and Globally? With travel bans, travel restrictions and major events being canceled, universities halting all events? How do you see that taking shape over the coming weeks?
Dr. Chen: Okay, so first of all, I have a live stream here. So it's actually most of them don't come back, right now it's only down about less than 2%. Okay, so that's good news because, in the morning, it was down 10%. So I'm glad mostly.
Thom Canalichio: So my numbers are delayed because I'm just looking at it on Google and you're looking at instant right?
Dr. Chen: Yes.
Thom Canalichio: Gotcha.
Dr. Chen: Yeah, I track it too. I mean, since it's so fluid, so it's good for me too.
Thom Canalichio: So that's a huge swing then to be down almost 2000 and then and then back to only down 2%, big change.
Dr. Chen: Exactly, so the volatility has gone way off, the up and downs since Monday as just tremendous, okay. So in terms of people's activity, and clearly you can tell it has really bad consequences on the economy because we slow down our business activity, we're not creating as much value as well as from work this side, okay, from the consumer side, we don't consume as much anymore. We don't go to restaurants, okay, we don't buy cars anymore, because, at this juncture, you cannot even go out why do you need a car? So all the sort of imposing terms of supply in terms of going to work be productive, as well as a consumer to consume to spend to create value, both of this channel was sort of effective. So if China is any sort of example we can tell that actually, you know, the economies are going way down. So in this sort of lockdown period of time, generally it's just gone way down. So I don't think we're there yet but you can see that it's good to have some consequences and also because of the government activity as I said earlier, okay. So we also have huge uncertainty about what the government will do, in particular, Trump will do. That uncertainty, you don't know what's the next activity is going to take uncertainty is going to hurt investors’ confidence too.
Thom Canalichio: In looking at the global economy, and International Trade, if we were to see prolonged impacts on the US economy that resulted in lower demand for manufactured goods, for example, coming from China, if those sorts of things were to really be in place for some time, are there other major long-lasting impacts that you'd see in terms of changes to what all of our intertwined economies around the globe are doing in terms of supply and demand for goods and manufacturing?
Dr. Chen: Okay, so right now, sort of the epicenter of this disease is moved out of China, moving to Europe here, so as a result, I think what you just described in terms of demand for Chinese exports, sort of [Inaudible 47:58] it already happened. So what happened in China, so as a response to this sort of lower demand, what happened is that the government [Inaudible 48:11] so they try to stimulate its consumption and spend within China to fill the gap of this demand deduction. So, as a result, they have all kinds of a big construction plan, which is going to play out in the open next [Inaudible 48:33]. So the government spending has gone really crazy and people are expecting other things to [Inaudible 48:42].
So in terms of long term view, I think the healthy development in China right now, I mean, not necessarily in terms of the consumption going up, is going to be good to the economy because eventually what happens is that it will spill over to other countries as in the US. So maybe the demand for US goods and also we should not forget the Trade War Treaty, okay because just conclude with one, China's agreed to buy around 200 billion goods. I think at this juncture it's perhaps a good thing for the US economy. For example, energy goods okay. So right now the demand for US energy good is so low because oil prices so low, so but because of agreement, so that would help [Inaudible 49:40] a little bit.
Thom Canalichio: Thank you and to Dr. Ewing. How do you view through the lens of history in these past outbreaks that you've studied, changes to the global economy as well as what other major steps that we should be taking now? And where do you see us in the course of the next maybe two to three months? On the basis of those previous models?
Dr. Ewing: Yeah, no, and I appreciate the question and also, listening to the comments from the panelists, reminds me of a conversation I've had half a dozen times today, which is, how is this what we're going through right now, similar to what we've experienced before and I don't think there was a close analogy to this recently, we had some disruption after the September 11 attacks, there were the H1N1 concerns in the spring of 2009, there was the economic crisis of 2008, but none of those, as far as I can tell, had the same kind of not only pervasive effect on society, but the mobilization of governments at every level to implement these kinds of really drastic measures. So I think we're in new territory right now and I think we need to recognize that, appreciate that. History can still be useful; I have to say that because it's just my profession if you look at the situation in the 1918 influenza epidemic, it comes to the United States in the middle of a war. The United States had been at war. The European powers are in their fourth year of the war and in some sense, the disease is overshadowed by that situation and its part of the reason there's less attention to the disease, in some cases in newspapers, the government is preoccupied. The United States government makes a decision, it's endorsed by President Wilson, to continue sending American troops across the Atlantic on these very tightly packed ship transports, where very, very large numbers of men got sick and many of them died. They were fully aware of the risks of that, but they decided the war effort was more significant it was more important to get man across the ocean to fight the war than it was to even recognizing the cost and so I think this reinforces the point that you've heard several times, which is, we have to deal with this disease, but we also have to recognize we're not dealing with it in isolation, we have all the contemporary global economic issues that we just talked about, their questions about how we're handling decisions at the federal government level at the state government level and in some sense, I agree with the sentiment that we need to put politics aside and just deal with the disease and absolutely endorse the idea of listening to the experts from the CDC and IAD and the WHO, but at the same time, we have to recognize that we don't choose the context in which we deal with these diseases and it has to be a factor in our consideration. So I think as I said earlier history gives us some guides that can help us identify things that work and avoid things that don't work but we also have to recognize this is an unprecedented situation that we're in. It's unprecedented in terms of the disease, but also our relationship with the media and our in the economic situation.
Thom Canalichio: Dr. Reyna, you have studied a lot about the aftermath of 911 something Dr. Ewing mentioned as a possible analog to kind of a monumental, transformative moment in our nation's history. I'm sure everyone recalls the sort of theme of that period being that everything changed. Does this measure up to a potential similar level of not only disruption to our daily lives, but looking forward and how people negotiate with these kinds of crises nationally and internationally? What are your thoughts on that?
Dr. Reyna: Well, I was in Washington, DC working at a research agency and met with a lot of people and was part of many Task Forces involving risk communication after 911 and how the government was communicating with people and I think there are many lessons to draw from that situation to now. Many of the scientific principles that some of our great scientists have developed, were implemented then and they apply now and that's the beauty of theoretical scientific principles. They have broad implications for different situations in different contexts. I would say, we really have to think about also, we really need to value our competent can-do people, our scientists, and our innovators. We need to think about if we're going to invest, for example, from the government, we can think about investing in things that will have long term payoffs, about infrastructure and so on, that will ultimately help the economy and humanity, so on later. So if we think very wisely about innovation and reinvestment and think in the long term, I think we'll be able to weather this better. We've got to think about our public health infrastructure and the comments on volatility are very instructive. We think about, well, the average use of the average emergency room, we may be equipped in many communities for that, but what about the variability? Can we handle these events that are going to stress the system? We have to think about that and plan ahead and I would say also, I want to underline that I think and please, the clinicians and epidemiologists correct me if I don't have this correct, social isolation and social distance, well, social distancing at this point has the capacity to flatten the curve and what that means is there will be community spread of the disease, but it will happen at a slower rate and that's very, very important because it means we won't necessarily exceed our capacity in hospitals and other things. So, notice, by the way, it's that categorical just above the capacity below the capacity. That's the key thing here. If we're able to keep it within the capacity of the health system to respond and meet people's needs, that means when people do get sick, they'll get care, and they're more likely to have good outcomes. So again, I think the social distancing is something we can do that will have multiple positive effects.
Thom Canalichio: Thank you, Dr. Reyna, I want to build on that response there with Dr. Dong and talk a little bit of what that capacity looks like and we've heard in some recent days of the situation in Italy, and with some of the communities that are being most hard hit, Doctors and hospitals are getting to the point of exceeding that capacity and having to make trade-off decisions for those who have the best outcome of potential survival, versus those who may not. One of the questions from one of our attendees, my mother is 88 and lives in an apartment, would she be safer if I brought her to live with me for a short time during the situation? As a geriatrician what are your thoughts about how families and communities can support those who are at risk? And obviously, if we were to make sure that the social distancing strategy was effective if they do need to then be admitted to an ICU, there's a bed for them. What are your thoughts about how someone can handle that? I'm sure there are a lot of people out there in the public asking the same question.
Dr. Dong: Sure, Thom, very reasonable, I think in general, that that type of support is needed, especially during this period of time, as a lot of psychological distress that's associated with this. It really depends on the risk level exposure for the family members. If older adults really could benefit from the support and minimize social isolation and the family is a fairly low risk, and I would say that that is very reasonable to have the elderly looked after but the at the same time if the family member is, for example, have high-risk exposures or who are in contact with sick patients who have potential higher risk, that that may or may not be in the best interest of older adults to have that family member moving with them, and really depends on what we call in geriatric medicine. What are the predisposing risk factors? What are the precipitating risk factors? And thinking about what is the risk factor of the older [Inaudible 58:46] that may put them at a low medium, high-level risk? And what are the [Inaudible 58:51] things that are outside of the control when you mix that together, really in geriatric medicine that is the combination that leads to our decision making on how to care and treat older adults if someone's really functional, and is happy living his or her apartment, and looking after them through social media through FaceTime, providing that support may be sufficient, as opposed to others who have more impairment in day to day activity daily living. In terms of infrastructure support, and I think as Dr. Khan said earlier, as we iterated if you don't feel well, if you're potentially sick, don't just go to the clinic or the emergency room without contacting your physician first. Don't put yourself and others at unnecessary risk. Hospitals are very much stressed, in this way, there's only limited to the intensive care unit beds or the step-down units, or the hospital beds in general and it's really important to be pre-emptive to think about not only how with the support the healthcare system with all necessary the missions, but rather from the family perspective, support older adults in different ways as well.
Thom Canalichio: Thank you, Doctor. If anyone else participating has questions for any of our experts, please do chat them to us and we will ask them. We're getting to about the hour mark and I want to move toward wrapping up shortly unless of course, we have more questions from media. While we're waiting to see if anyone chats any more questions, I do want to give every one of our experts an opportunity to answer this one question if you can, briefly. What is the key piece of misinformation that you've encountered during this that you would like to make sure is debunked unequivocally Dr. Dong?
Dr. Dong: Facemask, washing hands.
Thom Canalichio: That's the face mask is not effective, but washing hands is more effective?
Dr. Dong: Face masks are really not effective in terms of prevention for people who really have the disease and symptoms. Having face masks, the right kind of face mask is really important as well, but washing hands, how long to wash hands, is something which is often misunderstood as my earlier comment about singing Happy Birthday twice.
Thom Canalichio: Sing Happy Birthday twice. Yes, with the face mask, by the way, just a follow-up question to that if you may be sick, wearing a face mask, does that help you to reduce your risk of transmitting it to others?
Dr. Dong: It's not really the face mask; it's really how often we touch our face and nostrils area. That's really the part that people don't understand. If you wear the face mask that will potentially make things worse because you use the same one the bacteria virus may accumulate and that may actually potentially make you worse off than if you did not wear the face masks.
Thom Canalichio: Okay, noted and I'm sure a lot of people looking at buying face masks on Craigslist for $100 that maybe would like to know that. So thank you for that comment, sir. Dr. Khan is there a piece of misinformation that you've encountered recently that you'd like to make sure is unequivocally knocked down?
Dr. Khan: There are lots of pieces of misinformation and disinformation that I've encountered but let's just tell people to step away from the toilet paper and make sure that they actually buy food. So, let's make sure that everybody in our communities is ready. If they need to self-isolate for two weeks. That means, do they have sufficient food? Do they have sufficient water available to them? If they have the ability to their insurance company? Do they have their meds available to them, so they wouldn't need to go to a hospital to get their meds refilled? Do they make sure that they have good social contacts of who to contact and phone numbers to check up on them? So I think everybody should be putting together their preparedness plan and making sure that they're ready if they're really asked to quarantine because of potential exposure.
Thom Canalichio: Thank you, Dr. Chen, any myths, conspiracy theories or other misinformation you've encountered in your area that you'd like to address?
Dr. Chen: Well, I think I have alluded to before so in terms of the market and economic panic, we have experience, so I just want people to just look at history. So we have weather, as have talked about wet weather, almost all kinds since 911. We have weathered H1N1 and SARS in the long term stock market seems to be okay. Don't panic over the short term volatility.
Thom Canalichio: Don't panic over short term volatility. Thank you. Dr. Reyna, what about you? What's a key piece of misinformation that you'd like to comment on?
Dr. Reyna: Well, the key one is that the problem, the risk is low because there are so few people who've died at the moment and that is probably the single most dangerous piece of, it's not really a misconception because it's true, but it doesn't take into account as many misconceptions, it's kind of part of the truth, but it doesn't take into account this change and the fact that the probability is going to increase very rapidly and we have to think about the risk it's about the future and not about right now at this moment. Another misconception and misinformation that I think is very important to address is the whole issue of foreigners being the source of the disease, and that it's a hoax and things like that those kinds of ideas, along with distrust of the media are really kind of toxic soup for these kinds of crises and these are, again, short term issues, but also long term issues that we have to address.
Thom Canalichio: Thank you, Dr. Ewing, any thoughts about any misinformation, conspiracy theories or anything that you've seen that you'd like to raise as something that we should negate?
Dr. Ewing: Yeah, I think I would agree with many of the examples you've already heard. I think the one I would add goes back to something I was talking about earlier, and which many of us are dealing with right now. Which is the timing? The social distancing measures, I think it's a misconception to say we're going to wait to start to close schools or to shut down events or cancel sporting events until someone is sick by then it's probably too late for all the reasons we've just talked about in terms of how the disease is actually spread and I learned this from Twitter over the last few days social distancing is not for you. It's for everybody else. It's to keep you from infecting others and I think that's a change in mentality that we all need to embrace.
Thom Canalichio: Very good. Dr. Dong, you had mentioned to me that you wanted to address concerns about prejudice, discrimination, microaggressions toward Asians and the Asian American community as a result of this. We've seen this playing out in some news and social media. What do you have to say about that, and this might be one too that I'd like to open up to others on the team as we have obviously a diverse group but experts, what are your thoughts about that Dr. Dong?
Dr. Dong: Sure, we have seen quite a bit of xenophobia, xenophobia against Chinese and other groups in the US and around the world as well. When you look at Chinese history, the United States or one of the oldest immigrant groups who are one of the largest, and yet when you look at the history of Chinese Exclusion Act of 1882, the Anti-massage Nation Act during the Gold Rush period of time, and to what we face today and we've done our own research from the Pine study looking at discrimination. It's associated with all sorts of mental health outcomes as well as increasing risk for pre-mature death as well as increased risk for suicide. So I think it is something that we need to be very cognizant of is the issue of how we collectively as a community as social media, how we portray the stories, it's very human nature to think about this is something exotic and is coming to us as defined however we define that but it is something as a collective community we [Inaudible 1:06:59] to understand linguistic-cultural appropriateness and dealing with those kinds of issues.
Thom Canalichio: Thank you and Dr. Reyna, we've touched on this a little bit when we were speaking before the event. Is there anything about these kinds of issues discrimination, microaggressions, prejudice, against Asians?
Dr. Reyna: Yeah, I want to echo the prior remarks and we know from the scientific literature, that like this, this feeling of dread is going to increase and it will because the cases are going to increase exponentially. It is a psychological truism that people are going to look around for scapegoats. So, this will play into the narratives that we have currently going on, that people have with this distrust and beliefs about the other and we really have to, again, we have to think about this long term too. These are trading on long term fears of the other that are currently being activated but during a period of anxiety like this, we can expect them to increase and we gotta think proactively about communicating with people about these things.
Thom Canalichio: Thank you, Dr. Reyna, with that I think we will move to a conclusion. I'd love to tag my wonderful colleague Jessica Johnson to ask if she has any closing thoughts before we conclude.
Jessica Johnson: I want to thank everyone. This is a great panel. Thank you all for contributing and participating and yes, and for reporters and CIOs, and the audience, please feel free to contact us if you have any questions or other specific questions or other experts and sources. We are going to try to continue to have these events throughout the week. So we look forward to seeing you in the future.

APS Roundtable: Psychological Science and COVID-19, What We Know and What We Can Do
On March 18, the Association for Psychological Science convened a virtual roundtable of four APS members who discussed the psychological dimensions of COVID-19 and how it is affecting both society and individuals. The online gathering produced intriguing insights on the pandemic and the research-based actions we can take to minimize its impact.
Panelists included Bethany Teachman (University of Virginia), Katie McLaughlin (Harvard University), Valerie Reyna (Cornell University), and Andreas Olsson (Karolinska Institutet).
Before we begin, let us go around the virtual table and introduce ourselves and our particular areas of expertise.
I am Bethany Teachman, and I am a professor and director of clinical training at the University of Virginia in Charlottesville, and I think the primary reason I’m on the panel is that I study anxiety and emotion dysregulation and how people think differently when they’re anxious and what kinds of things we can do to try to manage that.
This is Katie McLaughlin. I’m a professor at Harvard University in the psychology department and my research focuses on how experiences of stress influence the way we think, our emotions, our ability to regulate our emotions, and our health.
I’m Valerie Reyna, a professor at Cornell University where I direct the Human Neuroscience Institute and I study risk communication and medical decision making. My research is about how people interpret the gist of risks, so that they can bring values to bear on their choices and lead healthy lives.
And I am Andreas Olsson, a professor at the Karolinska Institute in Sweden. I’m directing a lab with a research focus on fear and defensive behaviors. We are inspired by a cross-species approach with a focus on experimental work in humans, and we are particularly interested in how fear and anxiety spreads across individuals, which is termed social fear learning.
The COVID-19 pandemic can be seen as a “collective crisis.” Does this perspective change the way people adapt to and manage the situation?
Bethany Teachman: This is a situation that can have both positive and negative effects as a function of it being a collective crisis. On the positive side, there is a sense that we’re in it together and we see many amazing examples of people supporting one another. On the negative side, we see some people respond to this with a sense that they need to “protect their own” and it is “us versus them.”
Valerie Reyna: And many people are feeling both impulses at the same time. They’re obviously going to feel fear because of the uncertainty, the present threat, and the potential threats. And the social cues around people right now are going to raise their perception that we’re in danger. Then there’s the talk of the long-term impact to the economy too, and you have a real recipe for people to be anxious and frightened.
Andreas Olsson: The good side of this [being a collective crisis] is that sharing others’ anxieties and fears can motivate us to help each other, but the flip side is that sharing others' anxiety can cause a lot of suffering for some individuals. Today, when some people are monitoring the situation 24/7, that means they have exposure to a lot of suffering […] and this takes a big toll.
Katie McLaughlin: Psychological science has taught us quite clearly that in situations of mass trauma or mass stressors, like a natural disaster or a terrorist attack, there’s a very clear link between the degree of media exposure that people have and their symptoms of anxiety, depression, and substance abuse. People [should be] very mindful about how they’re engaging with media accounts of the virus in the current crisis and to try to limit exposure.
With the seemingly unrelenting stressors we are dealing with, is there a psychological equivalent to a low-grade fever that people may be experiencing?
Katie McLaughlin: This is unquestionably a period where people are experiencing an enormous amount of stress, given the large demands that the situation is placing on our daily lives—the changes in our routines and structures that we typically rely on, and the uncertainty surrounding how long this is going to last and what the ultimate impact is going to be on our families, on our communities, and on our workplaces. […] So absolutely, this is a period of time when people are likely going to be noticing higher levels of anxiety and depression than they might normally experience.
Bethany Teachman: It’s reasonable to have some anxiety and sadness. At the same time, it’s important not to get stuck there. There are a number of things that we can do to maintain as much of our normal lives as possible.
The first area is relationships. Social distancing does not have to equal social isolation. Those are two very different concepts and virtual interaction can make a big difference.
The second is thoughts and feelings. It really doesn’t help us to spend 10 hours a day scrolling through newsfeeds and posts on COVID-19. So in a number of anxiety treatments, we encourage people to pick a couple of times a day when they focus on their worries and get the information that they need to problem-solve but then spend the rest of their time living their lives as normally as possible.
The third piece is standard behavioral self-care. A lot of what helps at this time is healthy eating, sleep, exercise, and perspective-taking so that you don’t get stuck in assuming the worst.
And the fourth is to live your values. So be kind to yourself and be kind to others. This is a stressful time and anxiety is normal. We have to give ourselves permission to experience the feelings that we’re having and then to try to do as much as we can to maintain normality in the face of that situation.
Andreas Olsson: In the long run, if we would continue keeping up the vigilance and being stressed over time, this will definitely lead to a number of very bad consequences for us as individuals as well as society. We know that a long-term anxiety [can worsen attention spans], memory, and immune-system responses. So there’s a number of bad consequences in keeping this chronic anxiety for a longer period of time.
Katie McLaughlin: Social relationships are an incredibly important buffer against the negative consequences of stress. We know that having strong emotional support not only prevents anxiety and depression in periods of stress but also buffers against the negative physiological consequences of stress on the immune system and physical health. One of my very favorite studies shows that stress-buffering effects that you get from receiving social support you also get when you give social support to other people. And this is something that people can control right now—the degree of support they provide to others, including members of our communities who are more vulnerable.
Valerie Reyna: Human behavior is affecting everything from the stock market to the actions people take or don’t take to reduce risk, like social distancing. Behavior will determine the actual public health risk in the end. If we’re able to understand why behaviors are risky, and therefore follow appropriate guidelines, we will have a far better outcome than if we don’t.
From your experience, what is one thing psychological science tells us that we should know?
Valerie Reyna: One of the most important fundamental findings that informs what we’re dealing with right now is that people react to the gist of the events rather than the details and the facts. It’s how people interpret reality that governs their emotions and their actions, not the actual reality itself. So we have to think about this torrent of information washing over everybody. How can we help people extract the bottom-line gist of that information so that they can take effective action?
Bethany Teachman: We are not just passive recipients of what is happening. […] We can collectively work together to respond to this situation as a challenge, as opposed to appraising it as an impossible threat that we cannot manage.
Katie McLaughlin: Giving support to other people is just as effective at helping to reduce stress responses and the negative consequences of stress for our physical and mental health as receiving support from others.
We know very clearly that exposing yourself to a lot of media coverage about the pandemic is going to increase anxiety. The more we can create positive habits and boundaries around our exposure to media, the better.
Andreas Olsson: We not only have to understand our ability in our agency, but we also have to know the limitations of our minds. We really need to spend time trying to trust the experts. We have physicians and epidemiologists who are really good at explaining the effects of the virus on society. We also have psychologists who are really good at giving advice on how to cope with isolation, fear, and anxiety. In uncertain times like now, when it is impossible to have a full understanding of the situation, we need to rely on trusted sources of information.
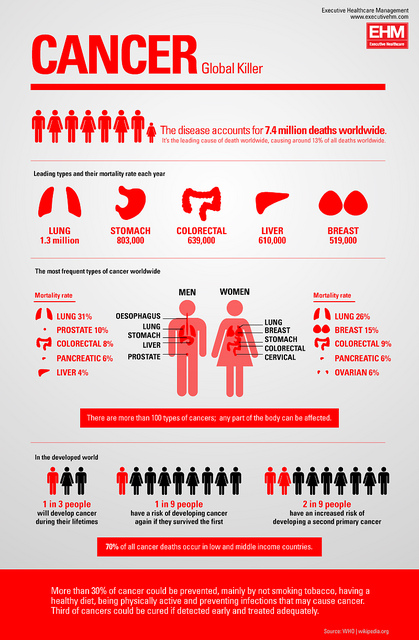 By H. Roger Segelken
By H. Roger SegelkenThe doctor says: “We offer two kinds of surgery for your cancer. Both procedures have 80 percent cure rates. After the first kind, 4 percent of patients have serious complications. In the second type, 20 percent simply die. No pressure to decide, but the sooner we start …”
Wishing you hadn’t slept through statistics class – trying to remember what went wrong with Uncle Joe’s surgery, and longing for the days when doctors knew best – you seek counsel in a decision-support tool, online or at the nearest cancer resource center.
“In fact, there are more than 40 tools to help people make informed decisions in cancer prevention, screening and treatment,” says Valerie F. Reyna, professor of human development in Cornell’s College of Human Ecology. “The more effective decision-support aids help with the numeracy problem – is a 10 percent chance riskier than one in a thousand? But not all tools help patients use their values, emotions and life experience to make decisions that affect their lives and their families’ future.”
Writing in the February-March 2015 special issue of American Psychologist, in an article titled “Decision Making and Cancer,” Reyna and her research colleagues want support tools to accommodate what they call “bottom-line gist options” that swirl though a patient’s mind – along with “verbatim” details about probable risk and whatever else the doctor said.
Gist is at the core of Fuzzy Trace Theory (which Reyna applied most recently to patients’ decisions to take antibiotics even though the misery is probably caused by viruses, not bacteria), and there’s nothing wrong with listening to one’s heart, Reyna says.
Reyna and her co-authors explain that “gist involves understanding meaning (insight in the gestalt sense) – integrating dimensions of information to distill its essence, not just processing fewer dimensions of information that are ‘good enough.’” Although people incorporate both verbatim details and gist in decision making, “they generally have a fuzzy processing (gist) preference” for information, the authors report.
The researchers offer this prescription for a Fuzzy Trace Theory-based cancer-decision tool: Ensure that patients understand the essential gist meaning of information; remind patients of an array of simple social and moral values that are important to them and that have relevance to the decision at hand; and assist patients in applying their values throughout the decision process.
“Every phase of the cancer continuum – from prevention, screening and diagnosis to treatment, survivorship and end of life – is fraught with challenges to our abilities to make informed decisions,” says Reyna. “People are not optimal decision makers. We struggle with complex information about benefits and risks, tradeoffs and uncertainties in cancer treatment.”
An impassionate computer could make optimal decisions on our behalf – disregarding the gist of what we think is best for us, Reyna adds. But the computer is too literal to make the best decisions for people, Reyna says: “Decision support should strive to capture the gist, the essential bottom line, of patients’ options.”
Reyna, director of the Human Neuroscience Institute in the College of Human Ecology, is the first author on the paper along with Wendy L. Nelson, National Cancer Institute; Paul K. Han, Maine Medical Center, Scarborough, Maine; and Michael P. Pignone, University of North Carolina at Chapel Hill.
Preparation of the American Psychologist report was supported, in part, by awards from the National Cancer Institute of the National Institutes of Health and the National Institute of Nursing Research.
By H. Roger Segelken
Reprinted from Cornell Chronicle, December 16, 2014

When the doctor says, “I could prescribe antibiotics for your sniffles, but it’s probably a virus – not bacterial,” do you decline? Many patients expect antibiotics, although overprescription is a major factor driving one of the biggest public health concerns today: antibiotic resistance.
Now researchers at Cornell, George Washington and Johns Hopkins universities have figured out why: “Patients choose antibiotics because there’s a chance [prescription medications] will make them better, and they perceive the risks of taking antibiotics as negligible,” says Cornell psychologist Valerie Reyna.
With her co-authors, the professor of human development has published new research with important implications for communicating about antibiotics: “Germs Are Germs, and Why Not Take a Risk? Patients’ Expectations for Prescribing Antibiotics in an Inner-City Emergency Department,” in the journal Medical Decision Making.
That’s encouraging news for health educators, Reyna says, noting: “Patients might expect doctors to prescribe antibiotics because patients confuse viruses and bacteria – and think antibiotics will be effective for either. Most educational campaigns attempt to educate patients about this misconception. However, we found fewer than half of patients in an urban ER agreeing with the message, ‘germs are germs.’”
Patients who understand the difference between viruses and bacteria – and take antibiotics anyway – are making a strategic risk assessment, Reyna says: “Our research suggests that antibiotic use boils down essentially to a choice between a negative status quo – sick for sure – versus taking antibiotics and maybe getting better. This risk strategy promotes antibiotic use, particularly when taking antibiotics is perceived as basically harmless.”
Fuzzy-trace theory
The Broniatowski-Klein-Reyna study is the first to apply “fuzzy-trace” theory to how people think about antibiotics. The theory predicts that patients make decisions based on the gist (or simple bottom line) of information.
As Reyna explains: “The goal is to make better decisions, getting antibiotics to patients who need them but not overusing them so the rest of the public is safe. Understanding how patients think is crucial because their expectations influence doctors’ decisions.”
Adds David Broniatowski, assistant professor of engineering management and systems engineering at GWU, and the report’s first author: “We need to fight fire with fire. If patients think that antibiotics can’t hurt, we can’t just focus on telling them that they probably have a virus. We need to let them know that antibiotics can have some pretty bad side effects, and that they will definitely not help cure a viral infection.”
The third author is Dr. Eili Klein, assistant professor in the Department of Emergency Medicine at the Johns Hopkins University and a fellow at the Center for Disease Dynamics, Economics and Policy.
Reyna is the director of the Human Neuroscience Institute, co-director of the Cornell University Magnetic Resonance Imaging Facility, and a co-director of the Center for Behavioral Economics and Decision Research, all in the College of Human Ecology. She is a developer of “fuzzy-trace theory,” a model of the relation between mental representations and decision making that has been widely applied in law, medicine and public health.
The study was supported, in part, by funds from the National Institutes of Health and the U.S. Department of Homeland Security.